Digital Health Decoded
Weekly news. Translational science perspectives.
All things Digital Health, decoded for you.
Powered by Beehiiv — no spam, unsubscribe anytime.
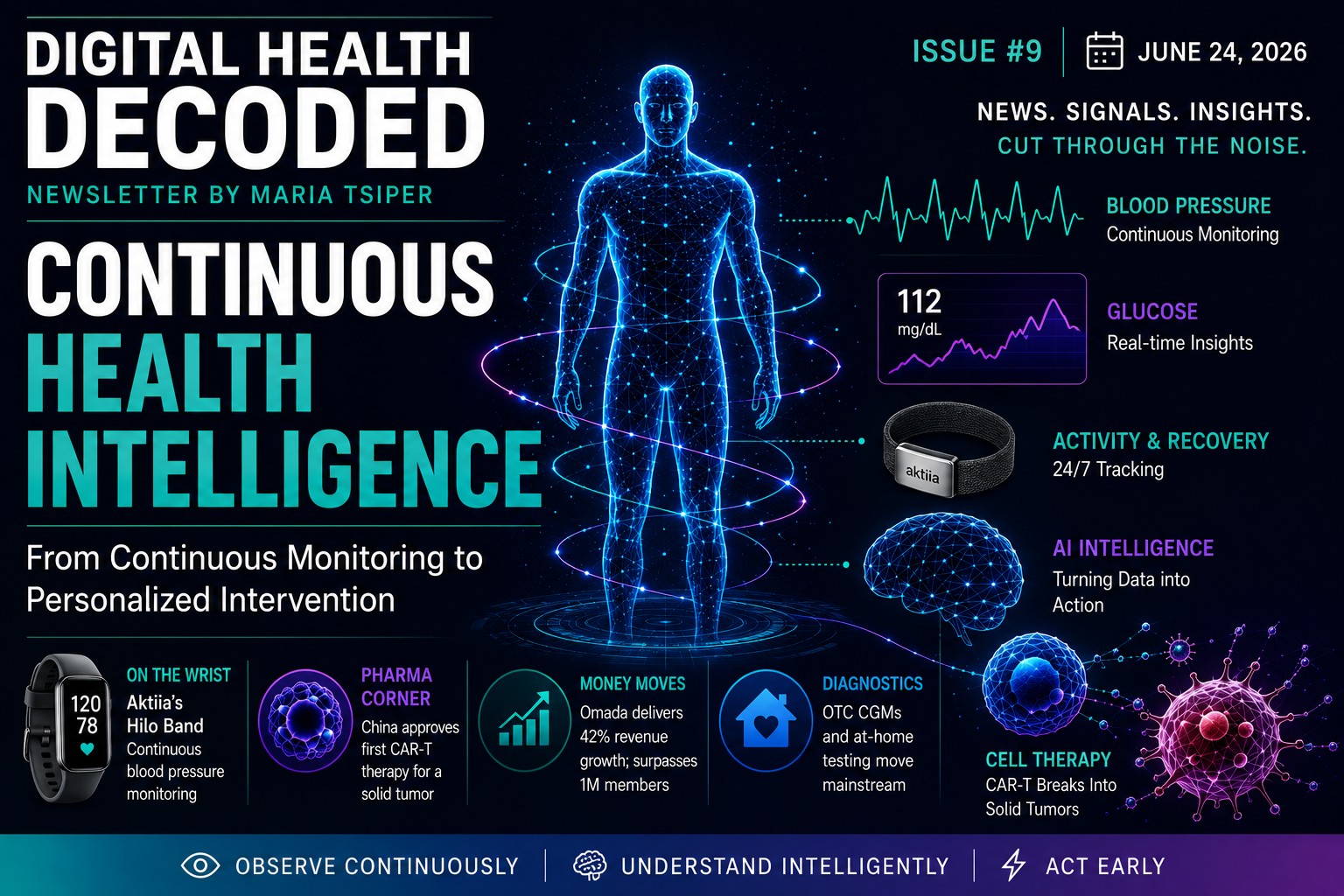
Continuous Health Intelligence
Cuffless BP and OTC glucose hit the shelves, the FDA reverses on Whoop, and China approves the first CAR-T for a solid tumor.
| # | Title | Read | Date |
|---|---|---|---|
| #9 | Continuous Health Intelligence Latest | 📄 On this site · Beehiiv → | June 24, 2026 |
| #8 | From the Plenary to the Patient | 📄 On this site · Beehiiv → | June 17, 2026 |
| #7 | Standards in Motion | 📄 On this site · Beehiiv → | May 27, 2026 |
| #6 | The Operating System for Human Health | 📄 On this site · Beehiiv → | May 20, 2026 |
| #5 | The New Front Doors | 📄 On this site · Beehiiv → | May 13, 2026 |
| #4 | Platforms, Not Products | 📄 On this site · Beehiiv → | May 6, 2026 |
| #3 | The Rise of “Closed-Loop” Pharma | 📄 On this site · Beehiiv → | Apr 23, 2026 |
| #2 | AI Moves Into Clinical Reality — and Security Becomes the New Battleground | 📄 On this site · Beehiiv → | Apr 16, 2026 |
| #1 | The Wearable Wellness Tech — Medical Device Convergence: What does this mean for your product? | 📄 On this site · Beehiiv → | Apr 9, 2026 |
Stay decoded.
Join readers getting the clearest signal in digital health — every Wednesday, free.
No spam. Unsubscribe anytime. Powered by Beehiiv.
⚡ Quick Hits
6 categories, 6–10 stories each week — curated from the best sources with Maria’s commentary baked in.
Funding, M&A & valuations
AI & ML in healthcare
Wearables & devices
Hospitals, telehealth & clinical ops
FDA, CMS & reimbursement
Drug development & biotech
💡 Maria’s Take
A candid, often provocative, expert perspective grounded in decades of translational science and commercialization experience.
📚 One Resource Worth Reading
A paper, report, or tool that Maria has personally reviewed and recommends — with context on why it matters.